Support COVID patients and informal caregivers from pre- to post-hospitalization
Project Overview
While health care professionals have gained more experience with the medical side of COVID-19 care, every patient and caregiver has been going through it for the first time, each time. Additionally, the need for social distancing means family caregivers can’t be at the bedside of the patient and absorb the intangible sensory information that can help them care for their loved ones post hospitalization. Partnering the HEART team and in collaboration with P&G, we created the COVID Caregiving Toolkit as a series of guides packed with advice and wisdom from COVID-19 patients & caregivers for COVID-19 patients & caregivers. These guides are available for anyone to use and for any hospital or health system to adapt.
My Role
Using a blend of human-centered design, lean thinking, and generative research as the backbone, my design team coached the HEART research team into being more deliberate about the choices they were making as they gathered information, recruited participants, and moved through the design process. We helped them navigate the ambiguity and bring clarity to a complex situation.
Outcomes and Impact
The series of 9 printable guides have been published for its patients by Michigan Medicine through their Office of Patient Experience (OPE). These guides are the most accessed resource on OPE’s website.
These guides are integrated into patient care at Michigan Medicine. They are available as resources for health care professionals through the Patient Education Clearinghouse, which includes materials that have been reviewed and approved by Michigan Medicine content experts for use during patient interactions.
Michigan Medicine is also launching a virtual, peer mentorship program to support COVID-19 caregivers and patients. These guides will form the backbone of this program.
These guides have been adapted by various other institutions in Michigan and across the nation.
We wouldn’t have been able to do this without the help of MICHR’s Translational Innovation team. MICHR was instrumental in helping to connect our research with a nuanced audience, understand their needs, and then create outcomes that really mattered to them. — Jeannette Jackson, MBA, Managing Director, HEART Project
Need
Caregiving for post-intensive care COVID-19 patients is an important determinant of successful recovery, including the likelihood of ICU readmission. However, the need for social distancing means family and friends can’t be at the bedside of the patient and absorb the intangible sensory information that can help them care for their loved ones post hospitalization.
As the pandemic progressed, health care professionals had gained increasing experience with the medical side of COVID-19 care, but every patient and caregiver has been going through it for the first time, each time.
I just became like a robot. I work full time. So I was home working remotely. I have two boys that were home. I knew what needed to get done, even though my feelings were still there. As long as I was busy doing something, I could get through the day. The phone was my lifeline. That’s how I learned updates on him. I couldn’t see him. I was at the mercy of the doctors that were treating him. It’s not like, ‘Oh, he has this disease. I’m going to call the best doctor to treat him.’ It’s just ‘this is what you’re getting’ and you pray he’s in good hands. And thankfully, they were able to fight for
him and he survived.
It was hard to navigate when he came home, to figure out what he would need. It’s a lot on the caregiver because everything falls on that person. Especially today when
people can’t be together. [My family was] there on the phone, but it’s not the same.
So you’re alone through all of this in so many ways. That’s probably the hardest part. Just trying to navigate and do everything on your own. It’s hard. It’s a lonely, frustrating feeling — a lot of running around and a lot of phone calls, a lot of trying to get the right answers and trying to get pointed in the right direction, no matter what it is — communication, insurance. It’s just always a lot of getting to really where you need to be. I have given everything to groom him and care for him. I became a caregiver.
— Spouse of a COVID-19 patient, December 2020
With possible ICU readmissions coinciding with a second wave of the pandemic, there existed an urgent need for an informed and deliberate intervention created for and by post-intensive care COVID-19 patients and their informal caregivers 1.
Process
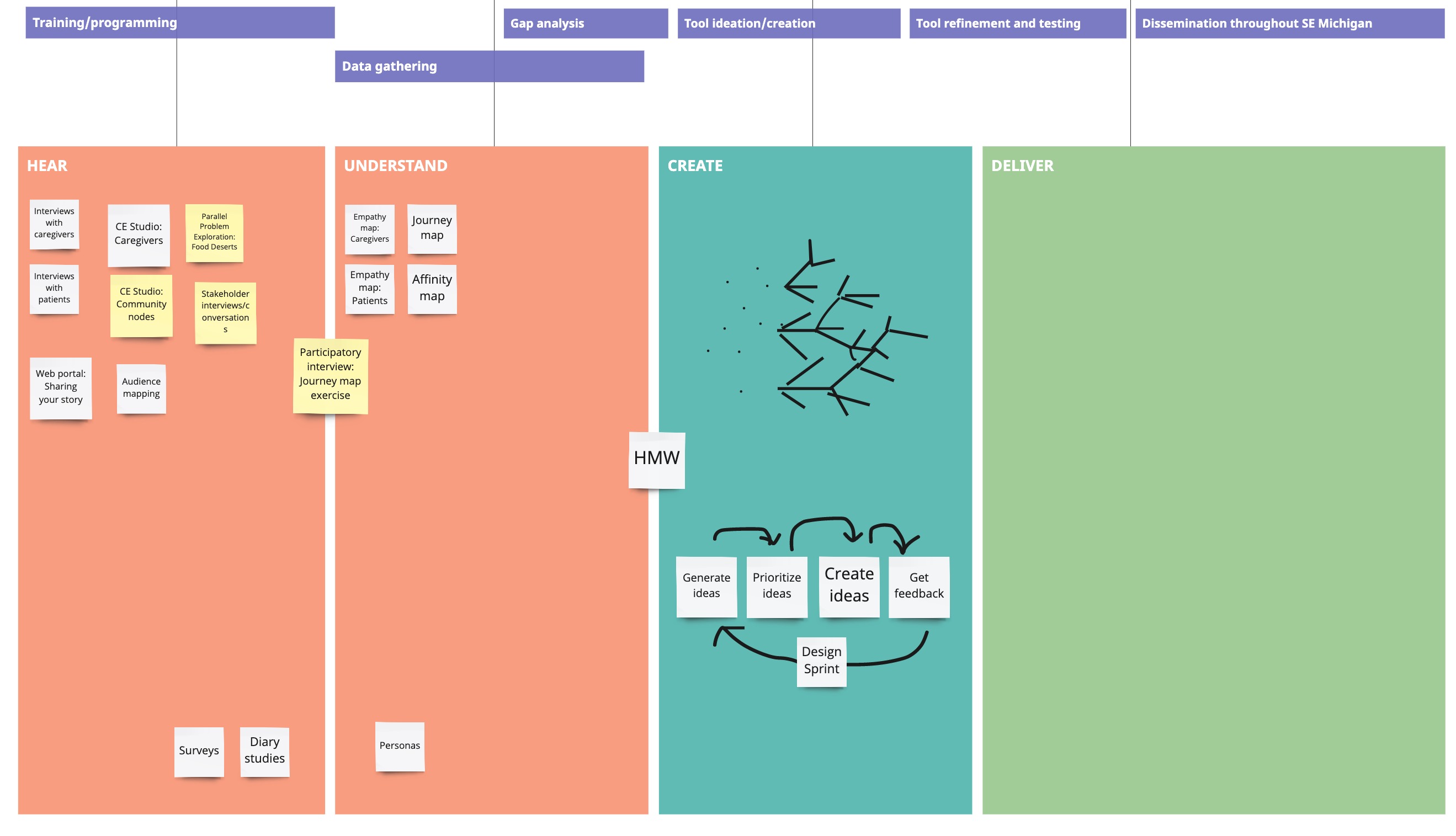
We helped the HEART team marry the linear academic research process with the need to be action-based and intervention driven. We started with understanding our users, creating a straw-man design, identifying assumptions and systematically bringing more clarity to an ambiguous situation.
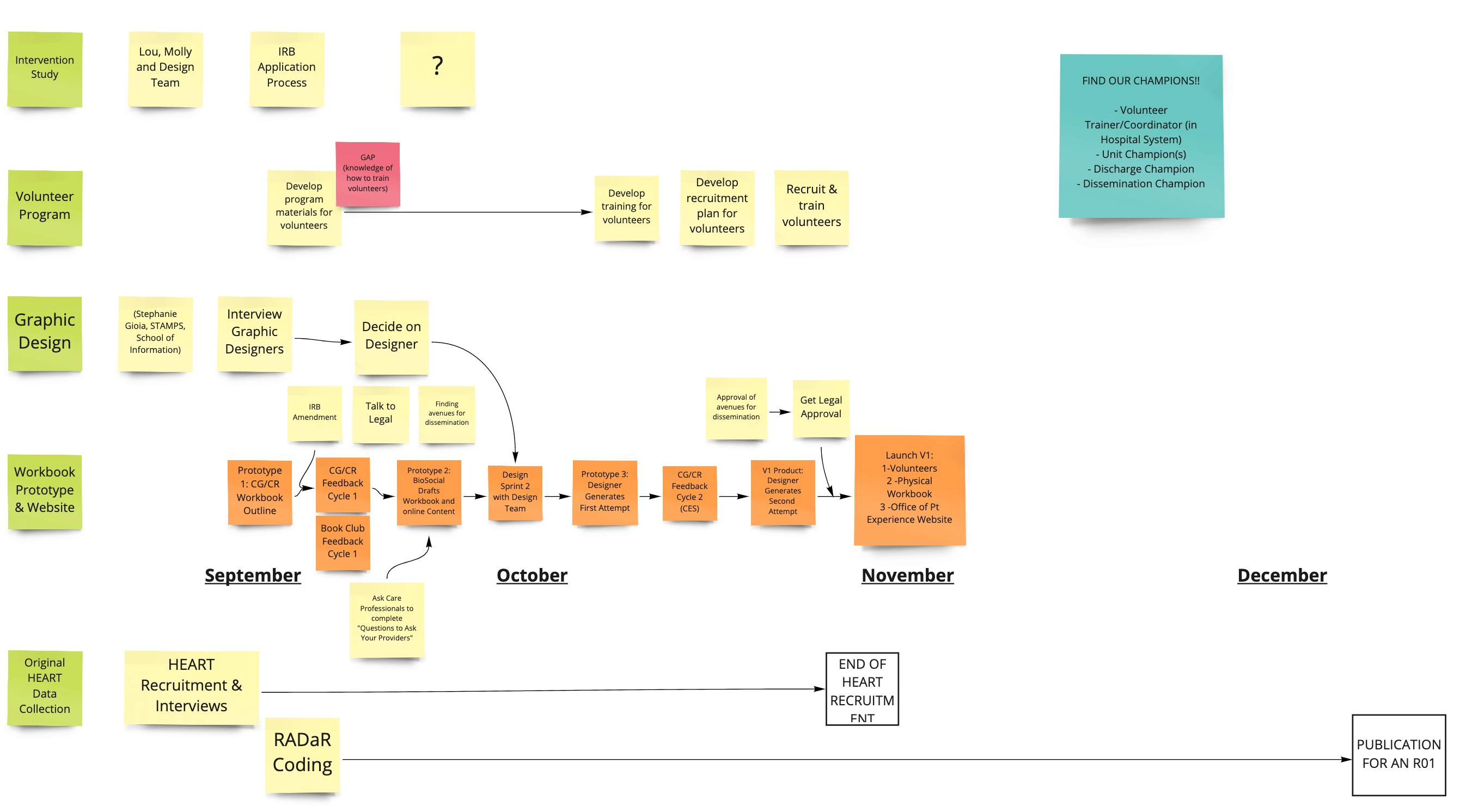
A snapshot in time depicting the process we hoped to follow. The process ended up roughly following along these broad steps.A timeline depicting some of the granular nuances of marrying the academic research process with that of human-centered design.
1. Identifying our audience
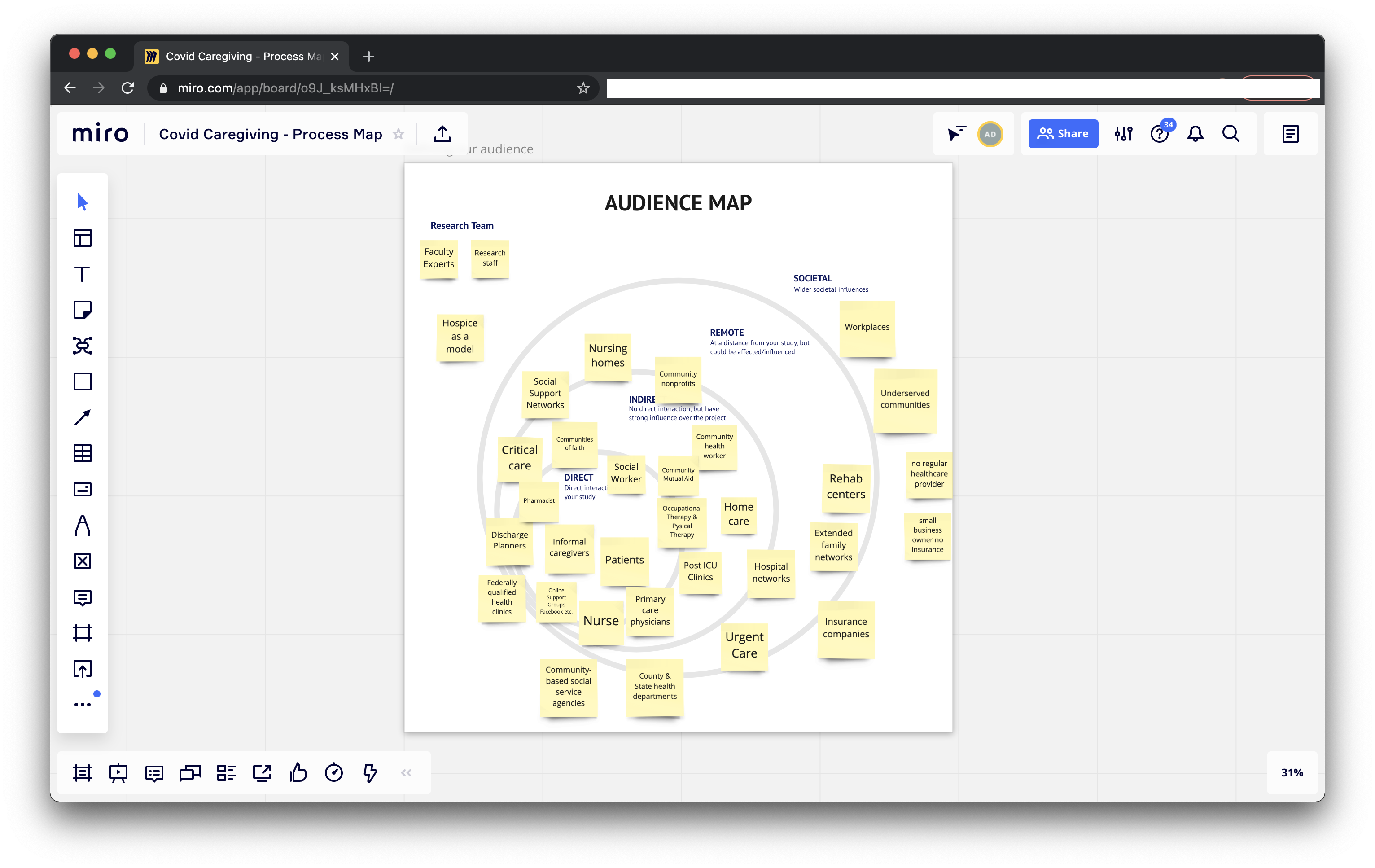
We worked with the core team to identify direct and in-direct audiences and start to get a sense of the people we were trying to impact. We realized that while patients and their loved ones were our primary audience, to get to them, we would have to engage with a variety of other stakeholders including doctors, nurses, social workers, check-in and check-out staff, faith leaders, nursing homes and county and state health departments.
An audience map allows teams to identify
and visually represent users/stakeholders and their relationships to each other and the project, process or organisation. Since this was 2020 and we had to all be remote, we used Miro as the tool to collaborate across disciplines.
2. Understanding our users
Through a comprehensive design research phase we then proceeded to gain insights into our users. This phase included
Individual interviews with patients and loved ones,
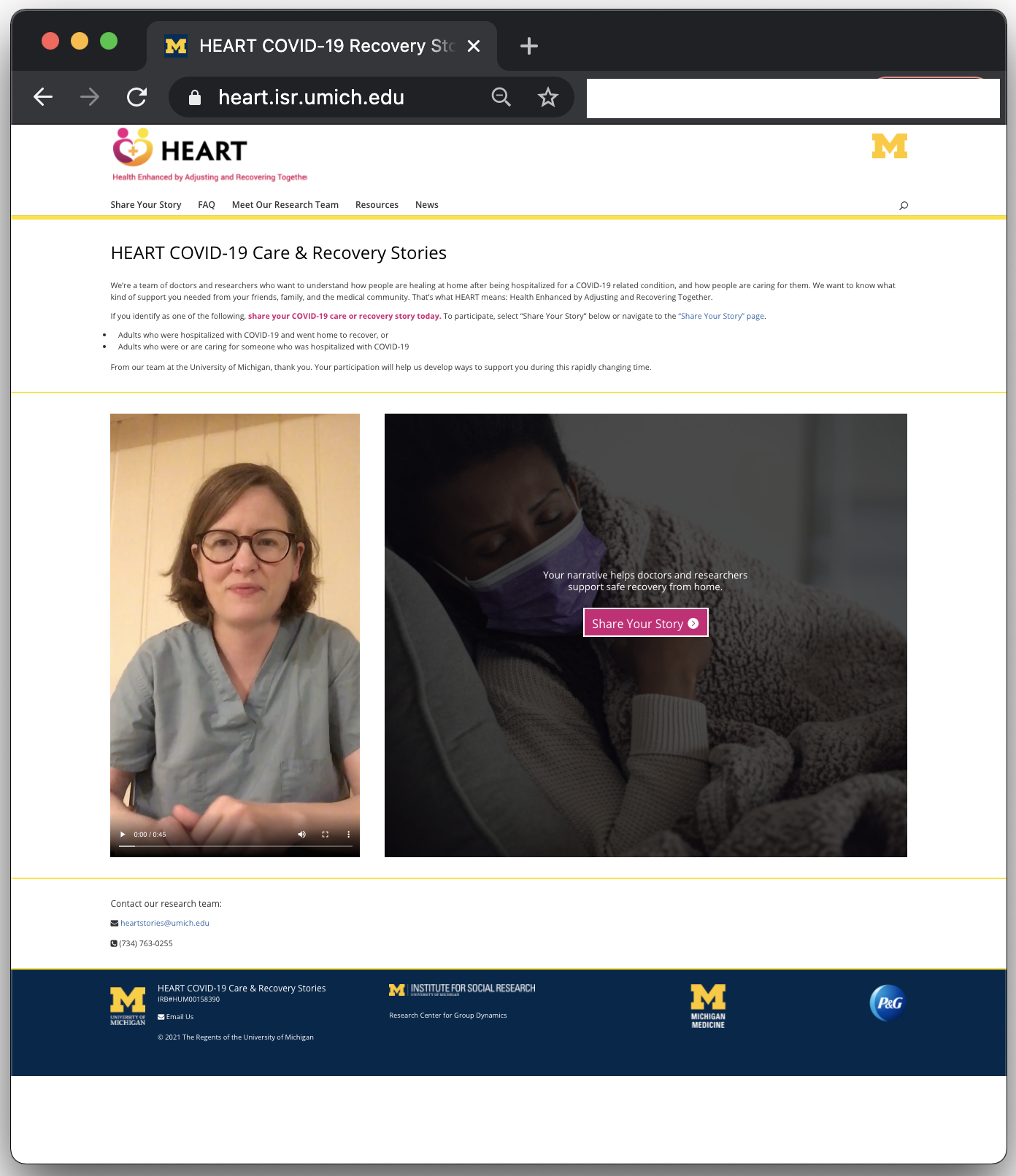
Launching an online platform that allowed patients and loved ones to share their stories either via text or by uploading a voice recording,
Journey mapping workshops conducted by the patients for the patients.
This generative, participatory, mixed-methods approach helped us gain a deep understanding of patients, loved ones and their COVID journey.
A screenshot of the online platform that empowered patients and loved ones to share their stories via text or video.
A screenshot from one of the Journey Mapping workshops that enabled patients and loved ones to share their stories.
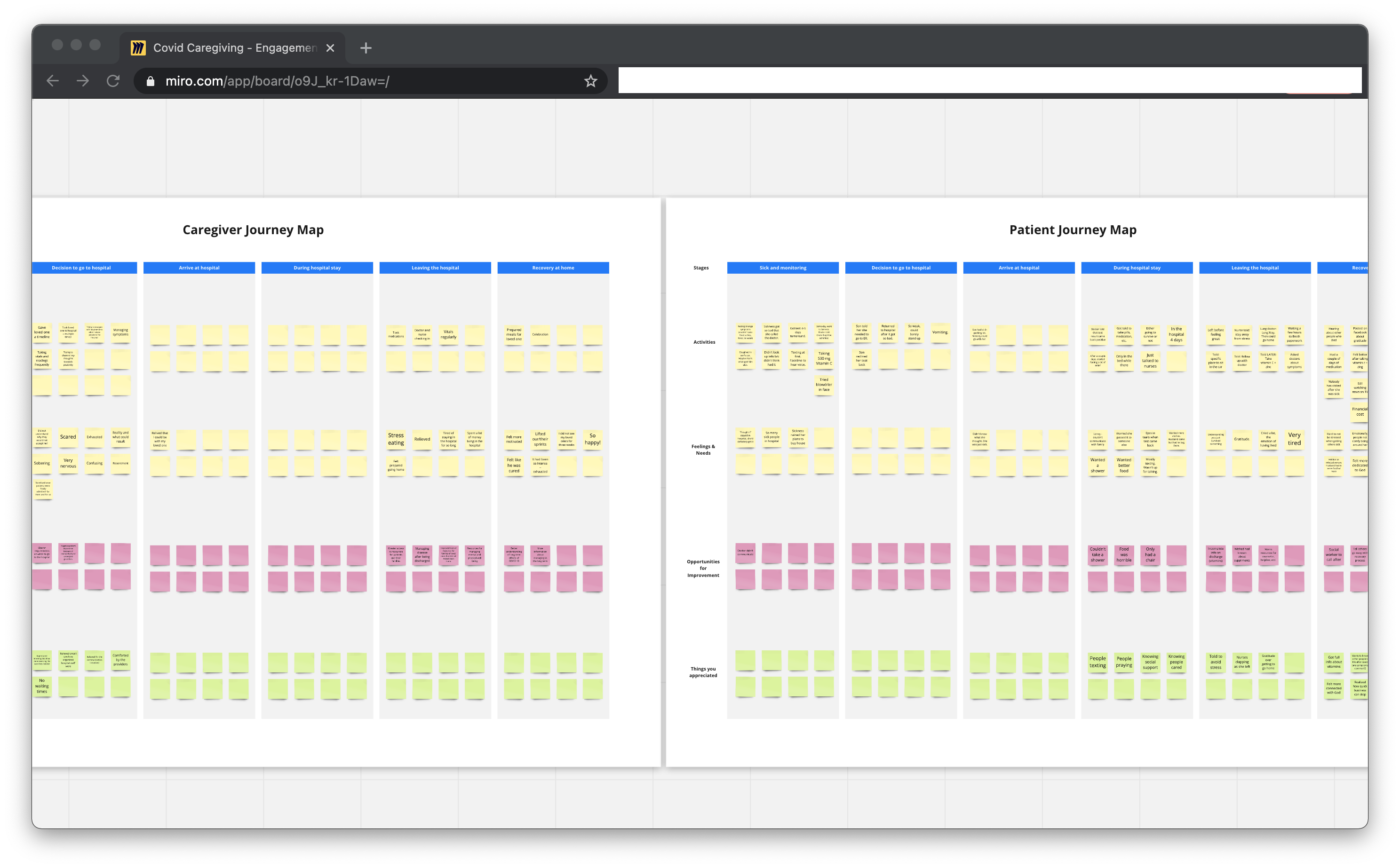
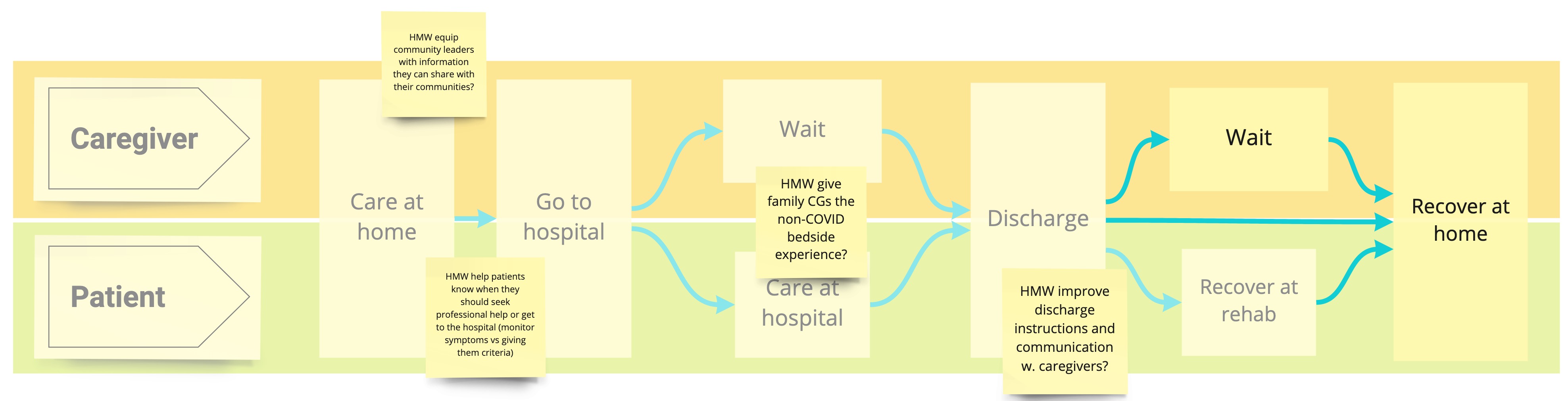
The insights gained from our research activities were visualized in a journey map. The journey map tracked patient and caregiver experiences along with potential opportunity areas through the following stages:
Sick and monitoring
Deciding to go the hospital
Arriving at the hospital
Hospital stay
Leaving the hospital
Recovering at home
The final journey map incorporating data from all our research mediums. This journey map served as a “boundary object” and helped our multi-disciplinary stakeholders collaborate effectively both on the problem, as well as the solution.
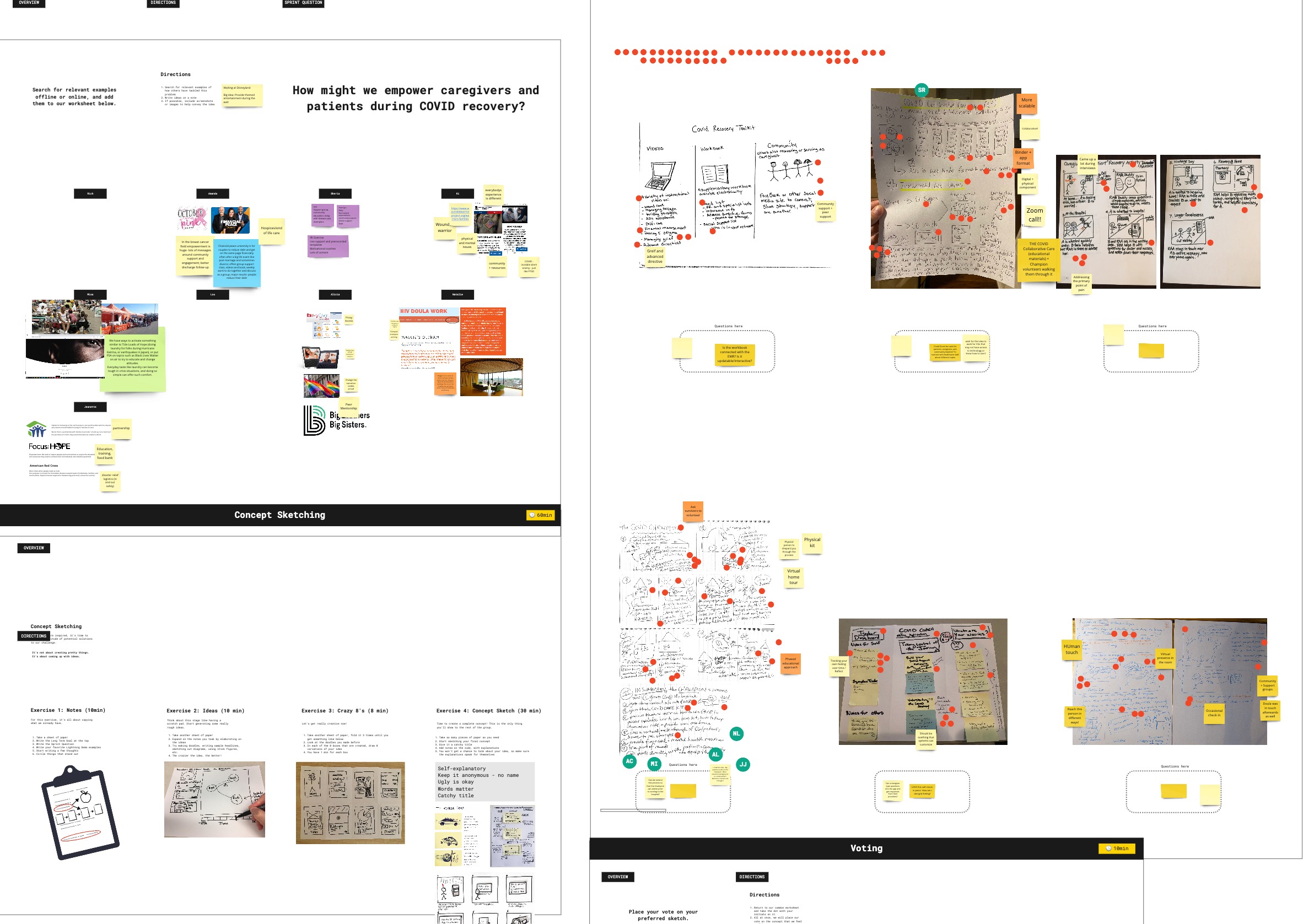
3. Setting up a design direction using a Design Sprint
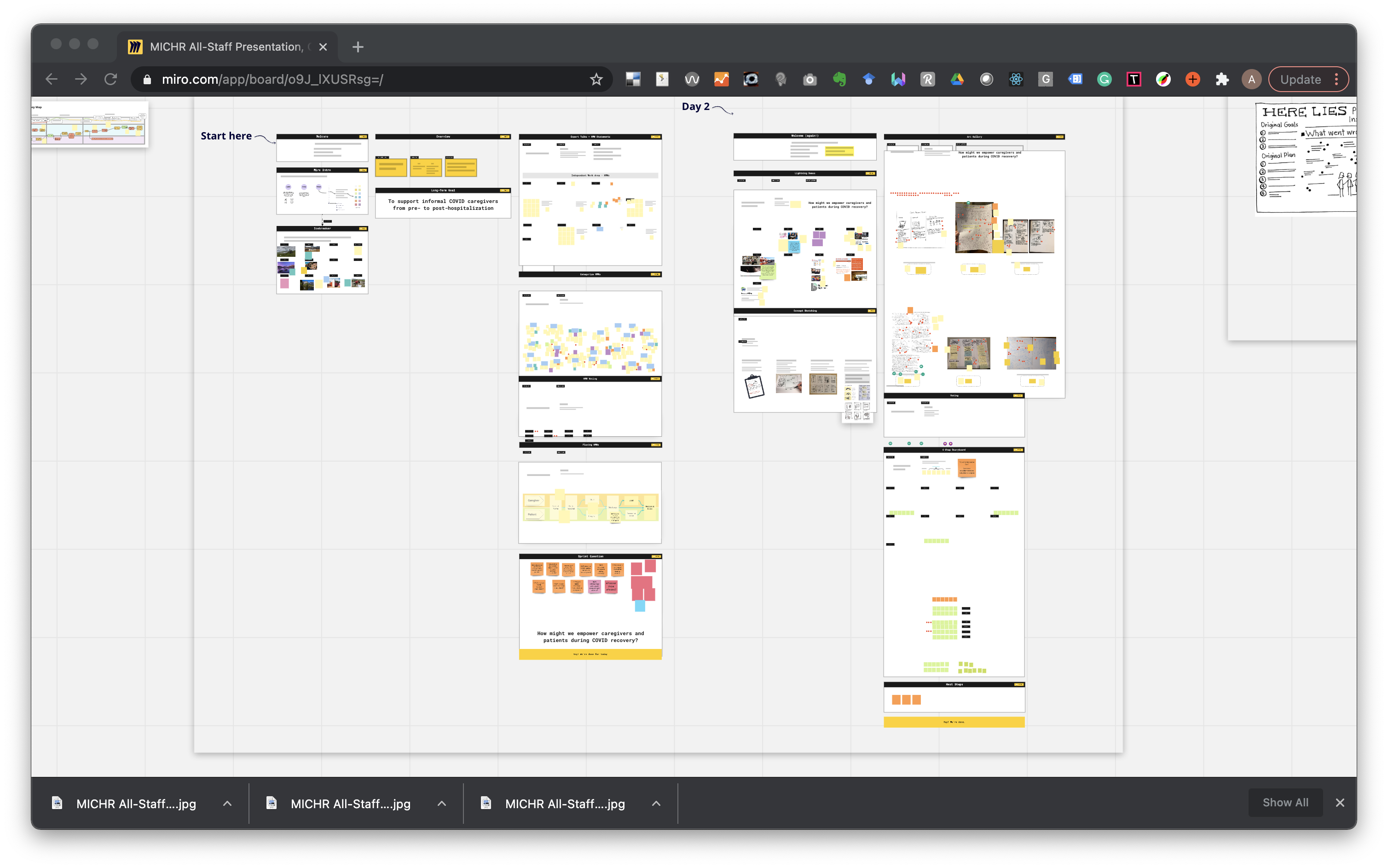
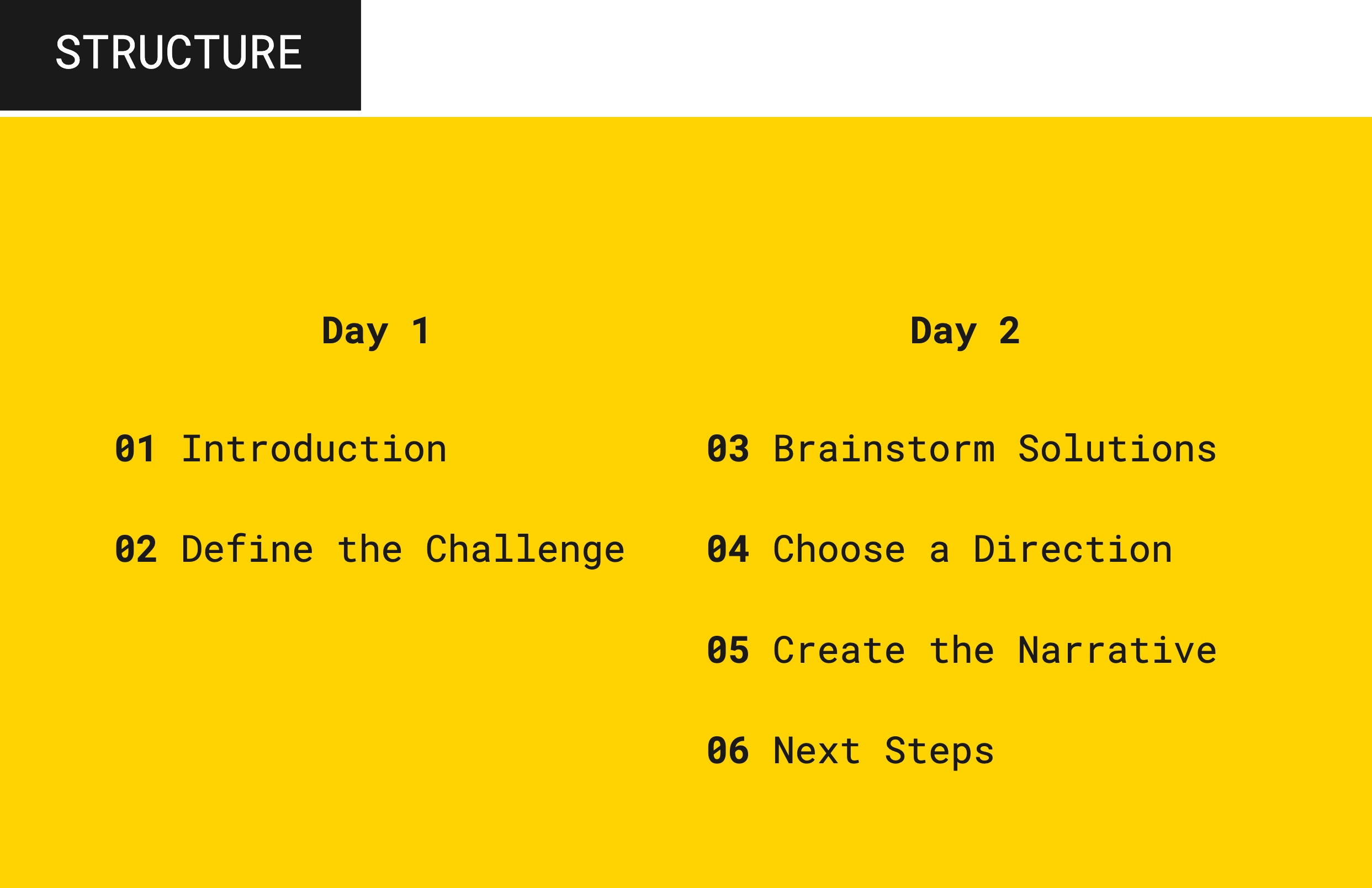
In order to jumpstart our creation process, we invited all stakeholders, including health-care providers, administrative staff, patients and caregivers, to join us for a two-day design sprint. By facilitating the design sprint, we helped jumpstart the design process by creating consensus around one (among many) potential direction to pursue — i.e. a straw-man that we could use to iterate further.
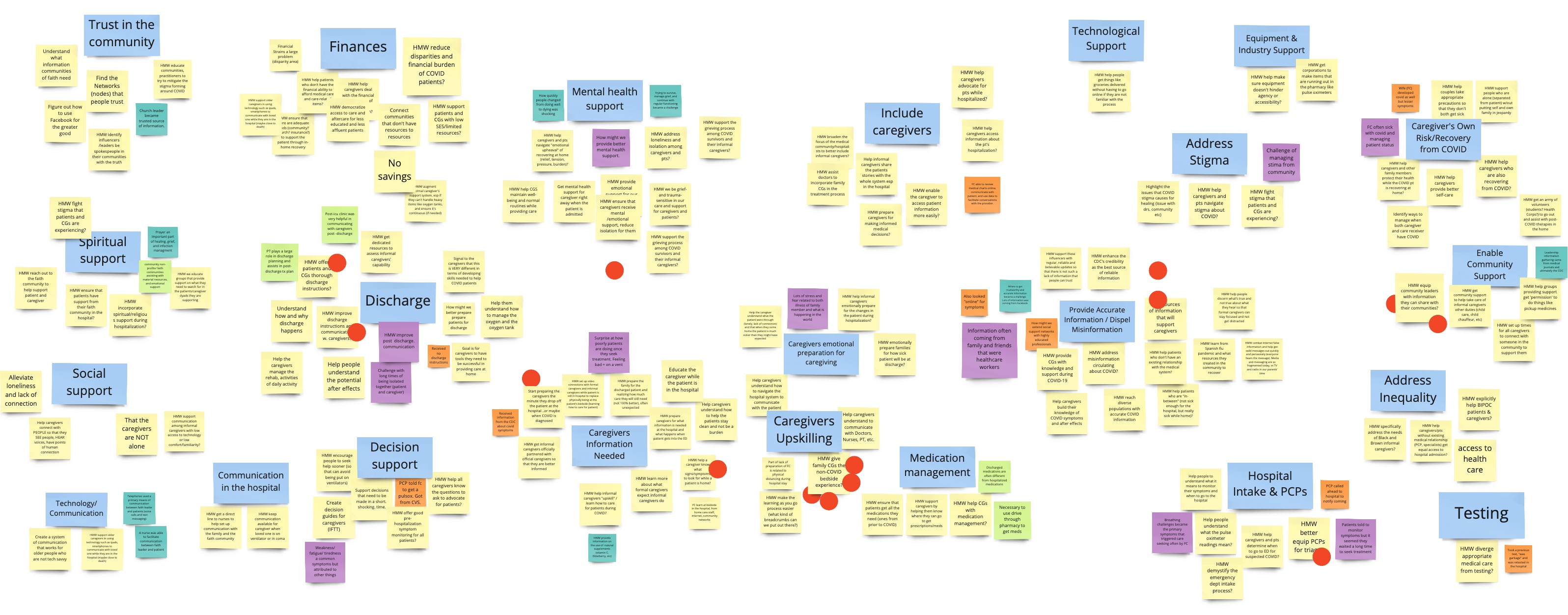
Screenshot from our remote design sprint that brought together health-care providers, administrative staff, patients and caregivers to build consensus on a design direction.Our design sprint was structured as a two half-day online event.A snapshot of potential “How Might We”s (HMWs) identified during the sprint.Identify points in the journey to target (day 1)Ideating during day 2
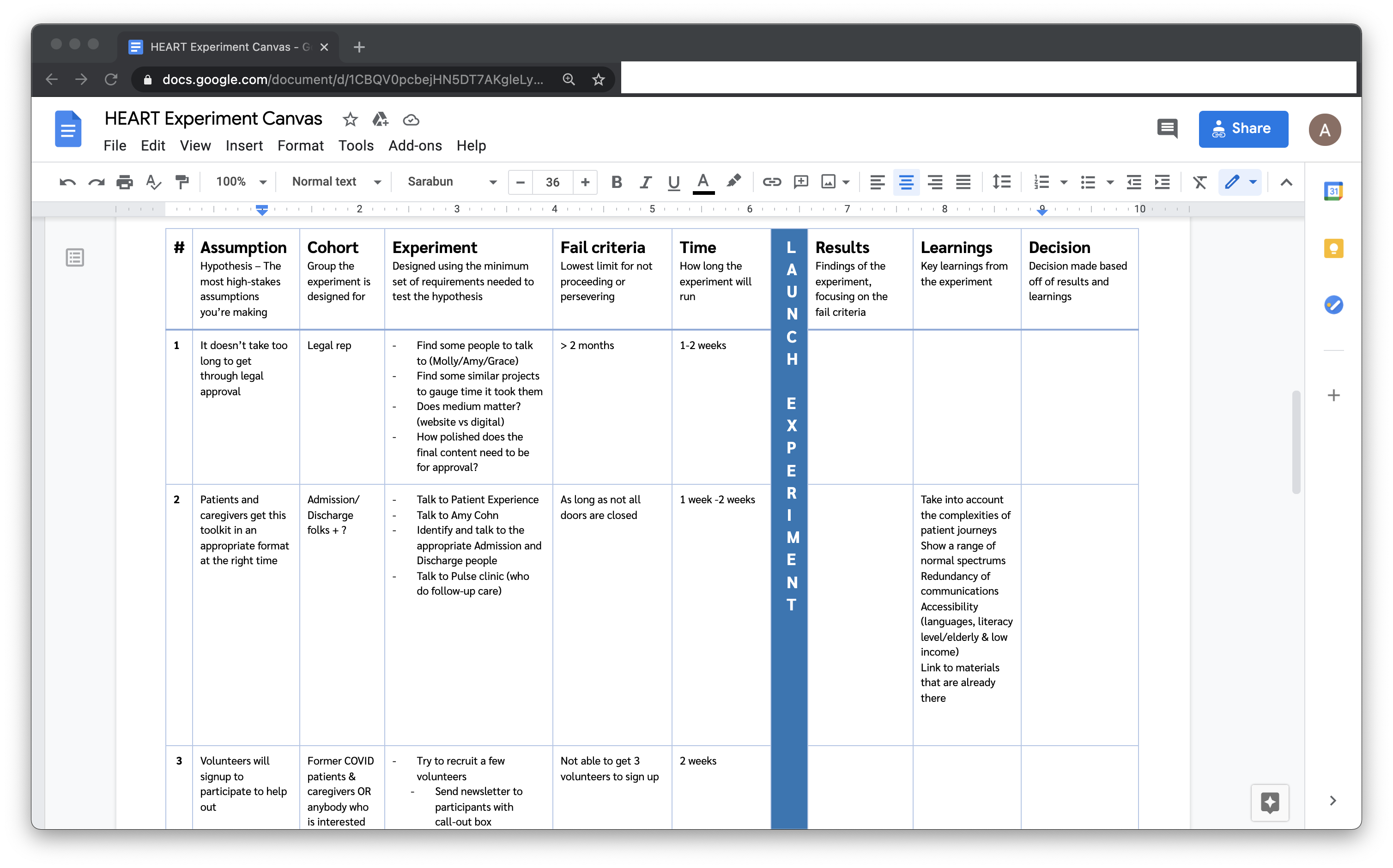
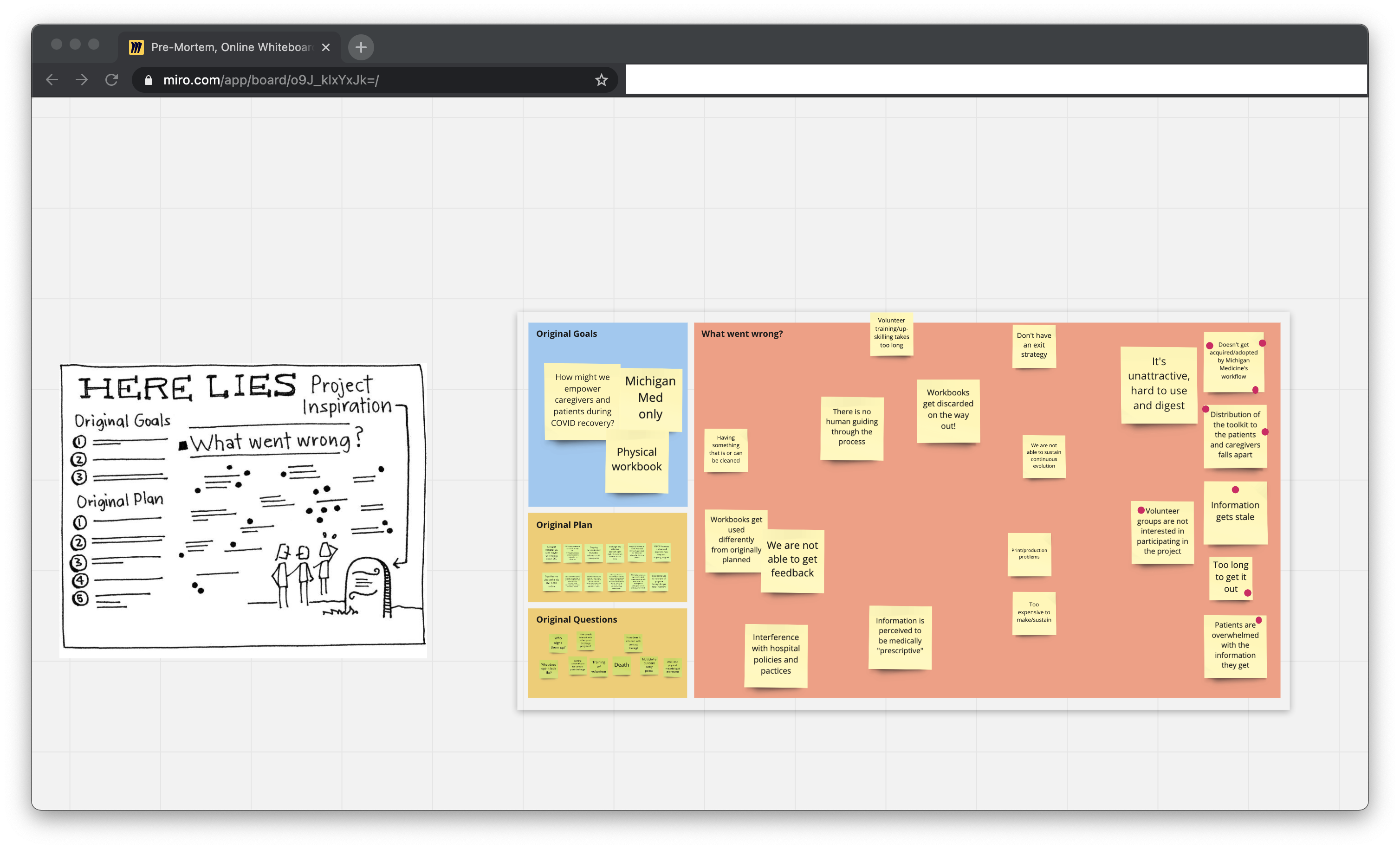
Once we had a handle on the direction we wanted to follow, we helped the HEART team identify inherent assumptions in the identified design direction. Some of the main assumptions identified included issues in content usefulness and usability (Example: Patients are overwhelmed with the information they get), distribution (Example: Toolkit Doesn’t get acquired/adopted by Michigan Medicine’s workflow) and interest (Example: Volunteer groups are not interested in participating in the project).
An experiment canvas mapping session
Pre-mortem in advance of one of the design iterations
Once we had identified our most critical assumptions, we went about systematically solving for them using an experiment canvas and subsequent design iterations. As an example, one of the assumptions we had built in was around the content of the toolkit. We used generative design methods that involved having patients improv situations with us leading to pointers on content that would be useful. Each iteration helped us further refine our solution, reducing the ambiguity and bringing increasing levels of clarity.
An Invision mockup used as the basis for a generative session with participants
5. Handoff, Service Incorporation, & Implementation
We helped the HEART team engage with stakeholders at the hospital to think through how the innovation could be adopted at an experiential level and into care. We helped them make connections into the department, helped them think through issues sustainability and resourcing as well as conducted several adoption and implementation workshops with various stakeholders.
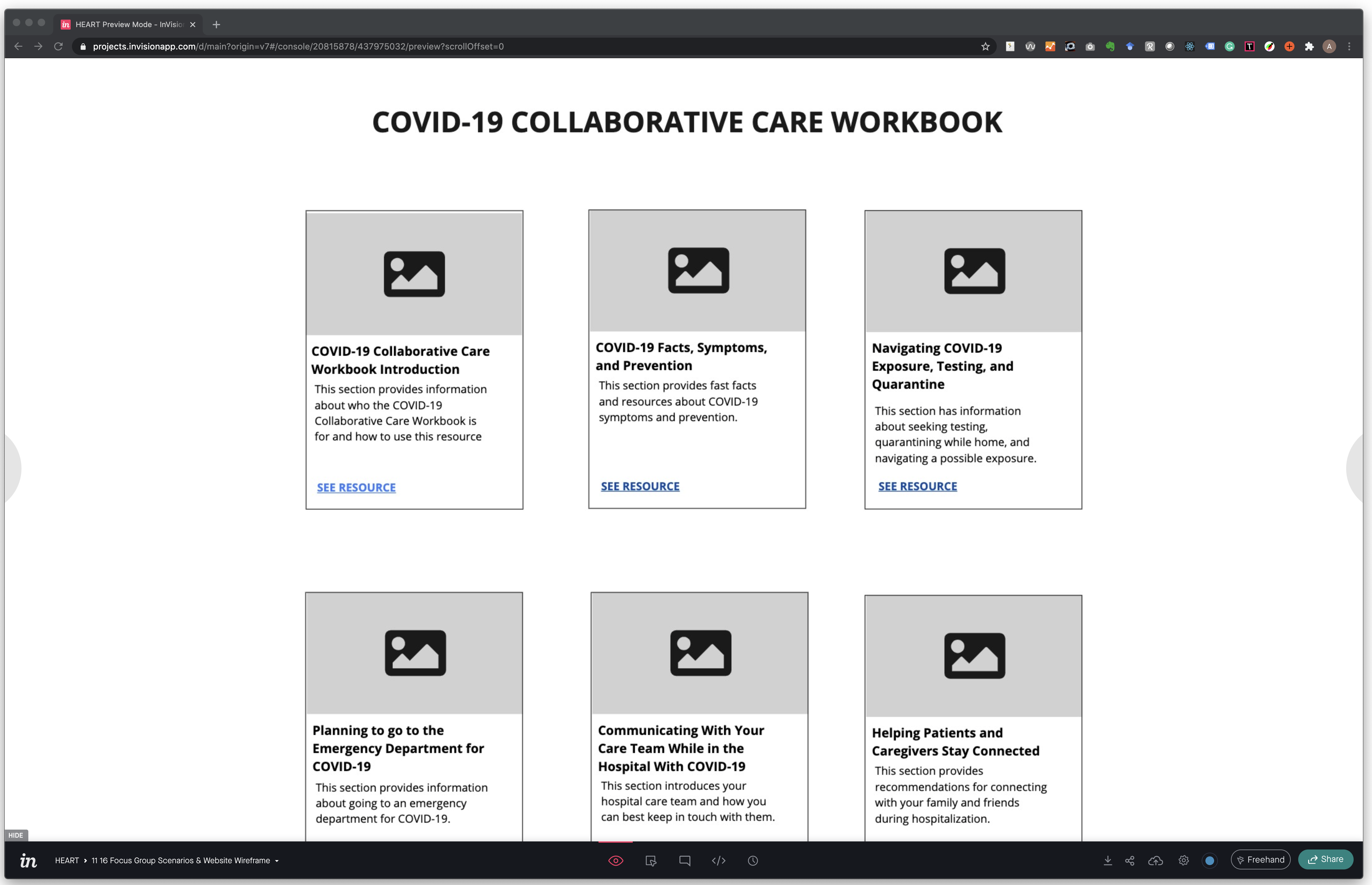
The COVID Caregiving Toolkit
A screenshot showing the first of 9 guides. The guides can be printed or used online.
The series of 9 printable guides have been published for its patients by Michigan Medicine through their Office of Patient Experience (OPE). These workbooks have valuable tips, links and more, as well as space to write down important information. Each guide focuses on a different part of the COVID journey:
Introduction: For all COVID-19 patients & caregivers
COVID-19 facts, symptoms, and prevention
Navigating COVID-19 exposure, testing, and quarantine
Preparing to go to the emergency department for COVID-19
Communicating with the care team while in the hospital with COVID-19
Helping patients & caregivers stay connected during COVID-19 (also includes tips for caregivers about loneliness and fatigue)
Preparing to go home after a COVID-19 hospital stay
Recovering at home after a COVID-19 hospital stay
Building your support network
The guides have approved for use during patient interactions and incorporated into the Patient Education Clearinghouse as resources for health care professionals.
Michigan Medicine is launching a virtual, peer mentorship program to support COVID-19 caregivers and patients. These guides will form the backbone of this program.
These guides are one of Michigan Medicine’s most accessed resources. These guides have also been adapted by various other institutions in Michigan and across the nation.